Children
Most people in American society resist associating the words children and death in a single phrase. They do not wish to contemplate the possibility that children may encounter death-related events either in their own lives or in the lives of others. As a result, they try not to think about the actual realities implied by the phrase "children and death" and they attempt to shield children from contact with or knowledge of such realities.
Although this effort at "misguided protectionism" is usually well meant, it is unlikely in most instances to be either successful or helpful. To explain why this is true, this entry explores how death and death-related events impinge on the lives of children and what their significance is for such lives. In addition, this entry considers the elements of a constructive, proactive program that helps children in their interactions with death and death-related events.
Children as Harbingers of the Future and Repositories of Hope
For many people in American society, children represent ongoing life and the promise of the future. In them, many hopes and ambitions are embodied. They foreshadow what is yet to come and act as a pledge of its surety. In a special way for females, they enter into life by emerging from their mothers' bodies. In addition, human children are vulnerable in special ways and for an unusually prolonged period of time. They call upon their adult caregivers to care for them. Their presence in adult lives is, more often than not, a source of pride and delight. As they grow and mature, children become their own persons and their parents' companions. In some cases, eventually they become caregivers of the adults who raised them. All these descriptions are true for one's natural children, as well as for those who are adopted or are foster children, and even when the latter are of a different ethnicity or culture.
Children, Adolescents, and Normative Development
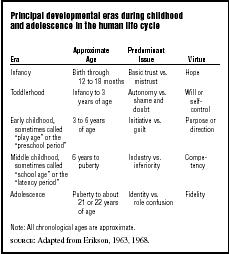
In the 1950s the psychoanalyst Erik Erikson proposed that there are four major eras (sometimes called "ages," "periods," or "stages") in the lives of children and an additional one for adolescents (see Table 1). His depiction of childhood has been highly influential to other developmental psychologists and scholars, although it is no longer universally accepted. Moreover, subsequent scholarship has sought to distinguish between three subperiods within adolescence. Still, a broad Eriksonian framework helps to draw attention to prominent aspects of physical, psychological, and social development in humans during childhood and adolescence, although it may not comment on spiritual development. Within limits, it can be useful as a general background for an overview of death in childhood and adolescence.
Erikson's model seeks to describe the normal and healthy development of an individual ego. It proposes that a predominant psychosocial issue or central conflict characterizes each era in human development. This is expressed as a struggle between a pair of alternative orientations, opposed tendencies, or attitudes toward life, the self, and other people. Successful resolution of each developmental struggle results in a leading virtue, a particular strength or quality of ego functioning. For Erikson, the task work in these developmental struggles is associated with normative life events, those that are expected to occur at a certain time, in a certain relationship to other life events, with predictability, and to most if not all of the members of a developmental group or cohort. This developmental framework is only roughly correlated with chronological age. Further, it might not apply at all or might only have limited relevance to individuals within different familial, cultural, and societal groups, and it might only apply uniformly to members of both genders when males and females are given equal options in life.
The importance of Erikson's work is the contrast between normative developmental events, however they may be described, and death-related events, primarily because most death-related events are nonnormative. They are unexpected or unforeseen events that occur atypically or unpredictably, with no apparent relationship to other life events, and to some but not all members of a developmental cohort. Still, nonnormative life events occur in a context of normative developmental events and each can influence the other in significant ways.
Both normative and nonnormative life events and transitions are life crises or turning points. They present "dangerous opportunities" that offer occasions for growth and maturation if an individual copes with them effectively, but also the potential for psychological harm and distorted or unsatisfactory development if the coping response is inappropriate or inadequate. Accordingly, the way in which a child or adolescent resolves the issue that dominates a particular era in his or her development and thereby does or does not establish its corresponding ego quality or virtue is likely to be relatively persistent or enduring throughout his or her life.
With respect to adolescence, various scholars have offered a fine-tuned account that distinguishes between three developmental subperiods, along with their predominant issues and corresponding virtues:
- • Early adolescence : separation (abandonment) versus reunion (safety); leading to a sense of emotional separation from dependency on parents
- • Middle adolescence : independence or autonomy versus dependence; leading to a sense of competency, mastery, and control
- • Late adolescence : closeness versus distance; leading to a sense of intimacy and commitment.
The Swiss developmental psychologist Jean Piaget looked at child development in a different way by focusing on processes involved in cognitive development during childhood. His work and later research on the development of death-related concepts in both childhood and adolescence is groundbreaking to the field of developmental psychology.
The various schemas all relay the fact that children and adolescents may encounter the deaths of others and even their own deaths. These and all other death-related events will be experienced within the ongoing processes of their own individual maturation. As the psychologist and gerontologist Robert Kastenbaum wrote in his article "Death and Development through the Life span": "Death is one of the central themes in human development throughout the life span. Death is not just our destination; it is a part of our 'getting there' as well" (Kastenbaum 1977, p. 43). Death-related events can affect human development during childhood and adolescence. Equally so, cognitive, psychological, biological, behavioral, social, and spiritual aspects
| Principal developmental eras during childhood and adolescence in the human life cycle | |||
| Era | Approximate Age | Predominant Issue | Virtue |
| Infancy | Birth through 12 to 18 months | Basic trust vs. mistrust | Hope |
| Toddlerhood | Infancy to 3 years of age | Autonomy vs. shame and doubt | Will or self-control |
| Early childhood, sometimes called "play age" or the "preschool period" | 3 to 6 years of age | Initiative vs. guilt | Purpose or direction |
| Middle childhood, sometimes called "school age" or the "latency period" | 6 years to puberty | Industry vs. inferiority | Competency |
| Adolescence | Puberty to about 21 or 22 years of age | Identity vs. role confusion | Fidelity |
| Note: All chronological ages are approximate. | |||
| SOURCE: Adapted from Erikson, 1963, 1968. | |||
of that development, along with life experiences and communications from the environment that surround children and adolescents, will all be influential in how they cope with intrusions into their lives by death. According to Kastenbaum, adults who help children and adolescents in this coping work need to be sensitive to the developmental context and the individual perspective of each child or adolescent in order to be successful.
Encounters with Death during Childhood and Adolescence
"'The kingdom where nobody dies,' as Edna St. Vincent Millay once described childhood, is the fantasy of grown-ups" (Kastenbaum 1973, p. 37). In fact, children and adolescents do die, and all young people can be and are affected by the dying and deaths of others around them.
The most dangerous time for children themselves is prior to birth (where they face the implications of miscarriage, stillbirth, and spontaneous or elective abortion), at birth (with all its risks of perinatal death), immediately after birth (with the potential perils of neonatal death), and during the first year of life. The best data available are for infant mortality. Data from the National Center for Health Statistics indicated that a total of 27,953 infants died in the United States during 1999. This figure represents 7.1 infant deaths for every 1,000 live births, the lowest rate ever recorded for the United States.
More than twenty other countries with a population of at least 2.5 million have lower infant mortality rates than those in the United States. Moreover, it is also true that infant mortality rates in the United States are nearly 2.4 times higher for African Americans (8,832 deaths or 14.2 per 1,000 live births) than those for non-Hispanic Caucasian Americans (13,555 deaths or 5.8 per 1,000) and Hispanic Americans (4,416 deaths or 5.8 per 1,000).
Congenital malformations, disorders related to short gestation and low birth weight, sudden infant death syndrome (SIDS), and maternal complications of pregnancy caused just under one-half (49.6%) of all infant deaths in the United States in 1999. There was a decline from 1988 to 1999 of 53.4 percent in the rate of SIDS deaths (from 140.1 to 65.3 per 100,000 live births). However, SIDS still remains the leading cause of death for infants between one month and one year of age, accounting for 28 percent of all deaths during that period.
Overall data on deaths and death rates during childhood and adolescence in the United States in 1999 are provided in Table 2, along with more specific data by age, sex, race, and Hispanic origin. (Note that racial and cultural categories overlap in the data presented in this table; thus, totals for all races are not identical with the sum of each subordinate category.) From Table 2 one can see that the largest numbers of deaths take place in infancy or the first year of life in childhood and in middle to late adolescence. In every age, racial, and cultural category, more males die than females, especially during middle and late adolescence. And in every age and gender category, death rates for African-American children are notably higher than those for non-Hispanic Caucasian Americans and Hispanic Americans. Death rates among Native-American children are typically lower than those for African-American children, but higher than for children in other racial and cultural groups—with the exception of fifteen- to twenty-four-year-old Native-American females who have the highest death rate in their age group. Death rates for Asian Americans and Pacific Islanders are uniformly lower than those for all other racial and cultural groups.
The leading cause of death in all children from one year of age through adolescence is accidents.

| Deaths and death rates (per 100,000) in the specified population group by age, sex, race, and Hispanic origin, United States, 1999 | ||||||||||||
| DEATHS | ||||||||||||
| Under 1 Year a | 1–4 Years | 5–14 Years | 15–24 Years | |||||||||
| Both Sexes | Males | Females | Both Sexes | Males | Females | Both Sexes | Males | Females | Both Sexes | Males | Females | |
| All races | 27,953 | 15,656 | 12,297 | 5,250 | 2,976 | 2,274 | 7,595 | 4,492 | 3,103 | 30,664 | 22,419 | 8,245 |
| Non-Hispanic Caucasian Americans | 13,555 | 7,722 | 5,833 | 2,820 | 1,606 | 1,214 | 4,488 | 2,643 | 1,845 | 17,869 | 12,678 | 5,191 |
| African Americans b | 8,832 | 4,899 | 3,933 | 1,309 | 745 | 564 | 1,789 | 1,096 | 693 | 7,065 | 5,350 | 1,715 |
| Hispanic Americans c | 4,416 | 2,411 | 2,005 | 883 | 482 | 401 | 1,014 | 592 | 422 | 4,509 | 3,549 | 960 |
| Asian Americans & Pacific Islanders b | 708 | 375 | 333 | 167 | 97 | 70 | 207 | 112 | 95 | 699 | 467 | 232 |
| Native Americans b | 344 | 180 | 164 | 82 | 48 | 34 | 105 | 55 | 50 | 540 | 396 | 144 |
| DEATH RATES | ||||||||||||
| Under 1 Year a | 1–4 Years | 5–14 Years | 15–24 Years | |||||||||
| Both Sexes | Males | Females | Both Sexes | Males | Females | Both Sexes | Males | Females | Both Sexes | Males | Females | |
| All races | 731.8 | 802.0 | 648.4 | 34.7 | 38.5 | 30.8 | 19.2 | 22.2 | 16.1 | 81.2 | 116.0 | 44.7 |
| Non-Hispanic Caucasian Americans | 572.7 | 636.8 | 505.4 | 29.7 | 33.0 | 26.2 | 17.5 | 20.1 | 14.8 | 71.4 | 98.7 | 42.6 |
| African Americans b | 1,552.8 | 1,694.6 | 1,406.2 | 58.8 | 65.9 | 51.4 | 28.7 | 34.6 | 22.6 | 123.1 | 185.7 | 60.0 |
| Hispanic Americans c | 612.0 | 655.3 | 567.0 | 32.2 | 34.4 | 29.8 | 16.9 | 19.4 | 14.4 | 82.4 | 125.0 | 36.5 |
| Asian Americans & Pacific Islanders b | 390.3 | 406.6 | 373.4 | 23.2 | 26.6 | 19.7 | 12.2 | 12.8 | 11.5 | 44.0 | 58.7 | 29.2 |
| Native Americans b | 808.6 | 839.5 | 777.3 | 51.4 | 59.4 | 43.1 | 22.4 | 23.1 | 21.7 | 125.9 | 183.5 | 67.5 |
| a Death rates are based on population estimates; they differ from infant mortality rates, which are based on live births. | ||||||||||||
| b Race and Hispanic origin are reported separately on death certificates. Data for persons of Hispanic origin are included in the data for each race group (unless otherwise specified), according to the decedent's reported race. | ||||||||||||
| c Includes all persons of Hispanic origin of any race. | ||||||||||||
| SOURCE : Adapted from Kochanek, Smith, and Anderson, 2001. | ||||||||||||
In children from one to four years of age, the second, third, and fourth leading causes of death are congenital malformations, cancer, and homicide. In children from five to fourteen years of age, the second, third, and fourth leading causes of death are cancer, homicide, and congenital malformations. In adolescents from fifteen to twenty-four years of age, the second and third leading causes of death are homicide and suicide, followed at some distance by cancer and heart disease.
Children encounter the deaths of others that are significant in their lives. Such deaths include those of grandparents or parents, siblings or peers, friends or neighbors, teachers and other school personnel, and pets or wild animals. Many adults undervalue the prevalence and importance of such deaths for children. However these experiences of childhood and adolescence can have immediate impact and long-term significance. Some prominent examples include the school shooting at Columbine High School in Colorado in April 1999, the countless instances of fantasized deaths and violence that children witness on television at an early age, and the many children who are members of families in which someone has died or is dying of AIDS (acquired immunodeficiency syndrome).
Children's Efforts to Understand Death
Children and adolescents are curious about the world around them. When death-related events intrude into their lives, they strive to understand them. Many factors affect such strivings, such as the intellectual capacities of the child, his or her life experiences, what society at large and adults around the child might say about the events, and the child's personality. Children's efforts to understand death may not always lead to thinking about death in the ways that adults do. It is incorrect to conclude from the way children respond to death that children have no concept of death or are never interested in the subject. To claim that "the child is so recently of the quick that there is little need in his spring-green world for an understanding of the dead" (Ross 1967, p. 250) is to be unfamiliar with the lives of children or to betray a personal difficulty in coping with death and a projection of those anxieties onto children. In reality children do try to make sense of death as they encounter it in their lives. According to Charles Corr, an educator who has written widely about issues related to children and death, such strivings should be aided by open communication and effective support from adults who love the child.
Expressions of Death-Related Attitudes in Games, Stories, and Literature for Children
Play is the main work of a child's life, and many childhood games are related to death. For example, little boys often stage car crashes or other scenes of violent destruction that they can manipulate and observe from a safe psychic distance, while little girls sometimes act out the ritual of a funeral or compare the deep sleep of a doll to death. Adah Maurer described peek-a-boo as a game in which the entire world (except, of course, the participating child) suddenly vanishes (is whisked away from the child's life) only to reappear subsequently in an act of instantaneous resurrection or rebirth. There is also the song in which "the worms crawl in, the worms crawl out," the lullaby "Rock-a-Bye Baby" that sings about the bough breaking and the cradle falling, and the child's prayer, "Now I lay me down to sleep," which petitions for safekeeping against death and other hazards of the night.
Similarly, children's oral and written fairy tales offer many examples of death-related events. For example, Little Red Riding Hood and her grandmother are eaten by the wicked wolf in the original version of the story, not saved by a passing woodsman or hunter. The Big Bad Wolf in the "Three Little Pigs" died in a scalding pot of hot water when the wolf fell down the last chimney. And while Hansel and Gretel escaped being shut up in a hot oven, the wicked witch did not.
There is a very large body of literature for children and adolescents that offers stories with death-related themes or seeks to explain death to young readers. Books range from simple picture books about children who find and bury a dead bird in the woods to more detailed stories that relay experiences involving the death of a beloved grandparent or pet, parent, sibling, or peer.
Children Who Are Coping with Life-Threatening Illnesses and Dying
Children with a life-threatening illness experience changes in their daily routines, acquire new information about their illnesses and themselves, and find themselves confronted with unexpected challenges. Many are anxious about those experiences, most need information that they can understand, and all need support as they make efforts to cope. In 1997 Michael Stevens, an Australian pediatric oncologist, suggested that the emotional needs of dying children include those of all children regardless of health, those that arise from the child's reaction to illness and admission to a hospital, and those that have to do with the child's concept of death. One twelve-year-old girl infected with HIV (human immunodeficiency virus) wrote: "Living with HIV and knowing that you can die from it is scary. . . . I think it is hardest in this order: Not knowing when this will happen. . . . Not knowing where it will happen. . . . Worrying about my family. . . . What will happen to my stuff and my room? . . . Thinking about what my friends will think" (Wiener, Best, and Pizzo 1994, p. 24).
Children Who Are Coping with Loss and Grief
Three central issues likely to be prominent in the experiences of bereaved children are: Did I cause the death?; Is it going to happen to me?; and Who is going to take care of me? These issues of causality, vulnerability, and safety cry out for clear explanations and support. In response, in 1988 Sandra Fox identified four tasks that are central to productive mourning for children: (1) to understand and try to make sense out of what is happening or has happened; (2) to express emotional and other strong responses to the present or anticipated loss; (3) to commemorate the life that has been lost through some formal or informal remembrance; and (4) to learn how to go on with living and loving.
When confronted with a death-related event, adults often try to block children's efforts to acquire information, express their feelings, obtain support, and learn to cope with sadness and loss. According to Charles Corr, this strategy cannot be helpful to a child in the long run because its effect is to abandon a child and its major lesson is that the child should not bring difficult issues to such an adult. By contrast, emotionally sensitive adults anticipate that sooner or later children need to turn to someone for help with death and loss. On that basis, they can try to prepare themselves for such moments, strive to ensure that they are responding to a child's real needs, try to communicate clearly and effectively, and work cooperatively with children, other adults, and relevant resources in society. This leads to a proactive program of helping that involves three elements: education, communication, and validation.
Experts note a good way to begin is with education; for example, by teaching children about death and loss in relatively safe encounters and by exploiting "teachable moments" for the insights they can offer and the dialogue they can stimulate. Next, one can turn to effective communication by asking three questions:
- What does a child need to know?
- What does a child want to know?
- What can a child understand?
Euphemisms and inconsistent or incomplete answers are not desirable because they easily lead to misunderstandings that may be more disturbing than the real facts. Honesty is dependable and encourages trust, the basis of all comforting relationships. So it is better to admit what you do not know than to make up explanations you really do not believe.
A third element of a proactive program is validation. Validation applies to children's questions, concepts, language, and feelings. It involves acknowledging these things in a nonjudgmental way and helping the child to name or articulate them so as to have power over them.
The advantages of a proactive program of education, communication, and validation can be seen in the examples of children who take part in funeral rituals and in support groups for the bereaved. Many adults in American society exclude children from funeral rituals, feeling that children might not be able to cope with such experiences and might be harmed by them. In fact, research has shown that taking part in funeral planning and funeral ritual in appropriate ways—not being forced to participate, being prepared ahead of time, given support during the event, and offered follow-up afterward—can help children with their grief work. Similarly, being given opportunities to interact and share experiences with others who are bereaved in the protected environment of a support group can help children and adolescents come to understand and learn to cope with death and grief.
Adult Children
One other sense in which the term "children" can be and is used in connection with death-related experiences has to do with adults who remain the children of their older, living parents. As average life expectancy increases in American society, growing numbers of middle-aged and elderly adults are alive when their children become adults. Indeed, some of the oldest members of American society, including the so-called old-old who are more than eighty-five or even one hundred years of age, may find themselves with living children who are also elderly adults.
Death-related events are relevant to these population groups in many ways. Among these, two stand out. First, when an adult child dies that may constitute a particular tragedy for a surviving parent. For example, the adult child may have been the primary care provider for the parent in his or her home, the only person to visit that parent in a long-term care facility, the individual who took care of practical matters such as handling finances or filling out tax forms for the parent, or the sole survivor from among the parent's family members, peers, and offspring. In these and other situations, the death of an adult child may impact the surviving parent in myriad ways, invoking losses and challenges in forms that had not hitherto been faced.
Second, the death of a parent at an advanced age who is survived by an adult child has its own spectrum of ramifications. Deaths of family members (especially parents) from an earlier generation often exert a "generational push" on younger survivors. These younger survivors, especially adult children, are now no longer "protected" in their own minds by their perceptions of the "natural order" of things. Previously, death may have seemed to them to be less of a personal threat as long as their parents and other members of an older generation remained alive. Now the adult children themselves are the members of the "oldest" generation. These adult children may be relieved of care giving responsibilities and other burdens that they had borne when their parents were alive, but new and often highly personalized challenges frequently arise for these adult children in their new roles as bereaved survivors.
See also: Children and Adolescents' Understanding of Death ; Children and Media Violence ; Literature for Children ; Suicide over the Life Span: Children
Bibliography
Balk, David E., and Charles A. Corr. "Adolescents, Developmental Tasks, and Encounters with Death and Bereavement." In Handbook of Adolescent Death and Bereavement. New York: Springer, 1996.
Blos, Peter. The Adolescent Passage: Developmental Issues. New York: International Universities Press, 1979.
Corr, Charles A. "Using Books to Help Children and Adolescents Cope with Death: Guidelines and Bibliography." In Kenneth J. Doka ed., Living with Grief: Children, Adolescents, and Loss. Washington, DC: Hospice Foundation of America, 2000.
Corr, Charles A. "What Do We Know About Grieving Children and Adolescents?" In Kenneth J. Doka ed., Living with Grief: Children, Adolescents, and Loss. Washington, DC: Hospice Foundation of America, 2000.
Corr, Charles A. "Children and Questions About Death." In Stephen Strack ed., Death and the Quest for Meaning: Essays in Honor of Herman Feifel. Northvale, NJ: Jason Aronson, 1996.
Corr, Charles A. "Children's Understandings of Death: Striving to Understand Death." In Kenneth J. Doka ed., Children Mourning, Mourning Children. Washington, DC: Hospice Foundation of America, 1995.
Corr, Charles A. "Children's Literature on Death." In Ann Armstrong-Dailey and Sarah Z. Goltzer eds., Hospice Care for Children. New York: Oxford University Press, 1993.
Erikson, Erik H. Childhood and Society, 2nd edition. New York: W. W. Norton, 1963.
Erikson, Erik H. Identity: Youth and Crisis. London: Faber & Faber, 1968.
Fleming, Stephen J., and Reba Adolph. "Helping Bereaved Adolescents: Needs and Responses." In Charles A. Corr and Joan N. McNeil eds., Adolescence and Death. New York: Springer, 1986.
Fox, Sandra S. Good Grief: Helping Groups of Children When a Friend Dies. Boston: New England Association for the Education of Young Children, 1988.
Kastenbaum, Robert. "Death and Development Through the Life Span." In Herman Feifel ed., New Meanings of Death. New York: McGraw-Hill, 1977.
Kastenbaum, Robert. "The Kingdom Where Nobody Dies." Saturday Review 56 (January 1973):33–38.
Kochanek, Kenneth D., Betty L. Smith, and Robert N. Anderson. "Deaths: Preliminary Data for 1999." National Vital Statistics Reports 49 (3). Hyattsville, MD: National Center for Health Statistics, 2001.
Metzgar, Margaret M., and Barbara C. Zick. "Building the Foundation: Preparation Before a Trauma." In Charles A. Corr and Donna M. Corr eds., Handbook of Childhood Death and Bereavement. New York: Springer, 1996.
Papalia, Diane E., S. W. Olds, and R. D. Feldman. Human Development, 8th edition. Boston: McGraw-Hill, 2000.
Papalia, Diane E., S. W. Olds, and R. D. Feldman. A Child's World: Infancy through Adolescence, 8th edition. Boston: McGraw-Hill, 1998.
Ross, Eulalie S. "Children's Books Relating to Death: A Discussion." In Earl A. Grollman ed., Explaining Death to Children. Boston: Beacon Press, 1967.
Silverman, Phyllis R., and J. William Worden. "Children's Understanding of Funeral Ritual." Omega: The Journal of Death and Dying 25 (1992):319–331.
Stevens, Michael M. "Psychological Adaptation of the Dying Child." In Derek Doyle, Geoffrey W. C. Hanks, and Neil MacDonald eds., Oxford Textbook of Palliative Medicine. New York: Oxford University Press, 1997.
Wiener, Lori S., Aprille Best, and Philip A. Pizzo comps., Be a Friend: Children Who Live with HIV Speak. Morton Grove, IL: Albert Whitman, 1994.
CHARLES A. CORR DONNA M. CORR
Comment about this article, ask questions, or add new information about this topic: