Abortion
Abortion is one of the most emotional and divisive moral issues of twenty-first-century American life. Consensus has not been reached on the numerous questions that swirl around the subject, including whether or not a woman has the right to choose a legal abortion, and under what conditions; the role of parents if she is not legally an adult; and the roles of the state and religion having veto power. In addition, the questions of when life begins and at what point it should be protected remain controversial.
Strictly defined, abortion is the expulsion or removal of an embryo or fetus from the uterus before it has developed sufficiently to survive outside the mother (before viability). As commonly used, the term abortion refers only to artificially induced expulsions caused by mechanical means or drugs. Spontaneous abortions occurring naturally and not artificially induced are commonly referred to as miscarriages.
Women choose to have abortions for a variety of reasons: They have had all the children they wish to have; want to delay the next birth; believe they are too young or too poor to raise a child; are estranged or on uneasy terms with their sexual partner; or they do not want a child while they are in school or working.
Artificially Induced Abortion around the World
Unplanned and unwanted pregnancies are common, and this fact fuels the controversy in every region of the world. Globally, more than one in four women who become pregnant have an abortion or an unwanted birth. In the developed countries of the world, including those in North America and Western Europe, where average desired family size is small, an estimated 49 percent of the 28 million pregnancies each year are unplanned and 36 percent of the total pregnancies end in abortion. In the developing countries, including parts of Eastern Europe, the Middle East, and Africa, where desirable family sizes are larger, an estimated 36 percent of the 182 million pregnancies each year are unplanned and 20 percent end in abortion.
Women worldwide commonly initiate sexual intercourse by age twenty, whether they are married or unmarried. In the developed countries, 77 percent have had intercourse by age twenty. This compares to 83 percent in sub-Saharan Africa and 56 percent in Latin America and the Caribbean. Couples in many countries have more children than they would like, or have a child at a time when they do not want one. The average woman in Kenya has six children, while the desired family size is four; the average Bangladeshi woman has four children but desires three.
From a global perspective, 46 million women have abortions each year; 78 percent of these live in developing countries and 22 percent live in developed countries. About 11 percent of all the women who have abortions live in Africa, 58 percent in Asia, 9 percent in Latin America and the Caribbean; 17 percent live in Europe, and the remaining 5 percent live elsewhere in the developed world.
Of the 46 million women who have abortions each year in the world, 26 million women have abortions legally and 20 million have abortions in countries where abortion is restricted or prohibited by law. For every 1,000 women of childbearing age in the world, each year 35 are estimated to have an induced abortion. The abortion rate for women in developed regions is 39 abortions per 1,000 women per year; in the developing regions the rate is 34 per 1,000 per year. Rates in Western Europe, the United States, and Canada are 10 to 23 per year.
Methods of Abortion
About 90 percent of abortions in the United States are performed in the first twelve weeks of the pregnancy. The type of procedure used for an abortion generally depends upon how many weeks the woman has been pregnant.
Medical induction. The drug mifepristone combined with misoprostol has been used widely in Europe for early abortions, and is now used routinely in the United States. Mifepristone blocks uterine absorption of the hormone progesterone, causing the uterine lining and any fertilized egg to shed. Combined with misoprostol two days later, which increases contractions of the uterus and helps expel the embryo, this method has fewer health risks than surgical abortion and is effective 95 percent of the time. Researchers in Europe report few serious medical problems associated with this method. Some of the side effects include cramping, abdominal pain, and bleeding like that of a heavy menstrual cycle.
Both pro-choice activists and pro-life activists see mifepristone with misoprostol as an important development in the abortion controversy. If abortion can be induced simply, safely, effectively, and privately, the nature of the controversy surrounding abortion will change dramatically. Clinics that perform abortions are regularly picketed by antiabortion protesters in the United States, making the experience of obtaining a legal abortion difficult for many women. If use of this method spreads in spite of opposition from antiabortion groups, abortion will become an almost invisible, personal, and relatively private act.
Vacuum aspiration. Also called vacuum suction or vacuum curettage, vacuum aspiration is an abortion method performed during the first trimester of pregnancy, up to twelve weeks from the beginning of the last menstrual period. It is the most common abortion procedure used during the first trimester in the United States, requiring a local or general anesthetic. The procedure takes about ten to fifteen minutes, although the woman stays in the doctor's office or hospital for a few hours afterward. Preparation for the procedure is similar to preparing for a pelvic examination. An instrument is then inserted into the vagina to dilate the opening to the cervix. The end of a nonflexible tube connected to a suction apparatus is inserted through the cervix into the uterus and the contents of the uterus, including fetal tissue, are then sucked out. Vacuum aspiration is simple and complications are rare and usually minor.
Dilation and curettage or dilation and evacuation. Dilation and curettage (D and C) is similar to vacuum aspiration but must be performed in a hospital under general anesthetic. It is performed between eight and twenty weeks after the last menstrual period. By the beginning of the second trimester of pregnancy, the uterus has enlarged and its walls have thinned. Its contents cannot be as easily removed by suction, and therefore the D and C procedure is used. The cervix is dilated and a sharp metal loop attached to the end of a long handle (the curette) is inserted into the uterus and used to scrape out the uterine contents. Dilation and evacuation (D and E) is a related procedure used between thirteen and sixteen weeks after the last menstrual period. D and E is similar to both D and C and vacuum aspiration, but is a bit more complicated and requires the use of forceps and suction.
Induced labor. For abortions later in the pregnancy (sixteen to twenty-four weeks), procedures are employed to render the fetus nonviable and induce delivery through the vagina. Only 1 percent of abortions in the United States are performed by inducing labor and a miscarriage. Because the woman experiences uterine contractions for several hours and then expels a lifeless fetus, these procedures are more physically uncomfortable and often more emotionally upsetting. The two most common procedures used in this period are prostaglandin-induced and saline-induced abortions. Prostaglandins can be injected directly into the amniotic sac through the abdominal well, injected intravenously into the woman, or inserted into the vagina as a suppository. They stimulate uterine contractions that lead to delivery. Saline (salt) solution can also be injected into the amniotic fluid and has a similar effect. Late-term abortions, also called partial-birth abortions by some, stir considerable controversy in the United States.
Hysterotomy. This extremely rare procedure, also performed from sixteen to twenty-four weeks after the woman's last menstrual period, is limited to cases in which a woman's uterus is so malformed that a D and E would be dangerous. In essence, a cesarean delivery is performed and the fetus is removed.
Methotrexate and Misoprostol. Because of social and political pressure from antiabortion activists, the number of obstetricians, gynecologists, and hospitals performing abortions in the United States has been steadily dropping, but this trend could change as doctors adopt a nonsurgical alternative using prescription drugs already marketed for other purposes. A combination of the drug methotrexate, which is toxic to the embryo, with misoprostol, which causes uterine contractions that expel the dead embryo, has been shown to be effective in inducing abortions at home.
The Abortion Issue in the United States
In 1973 the U.S. Supreme Court overturned by a 7–2 vote laws that had made abortion a criminal act. Since that decision by century's end approximately 21 million American women have chosen to have 35 million abortions. Researchers estimate that 49 percent of pregnancies among American women are unintended, and half of these are terminated by abortion. Forty-three percent of women in the United States will have at least one abortion by the time they reach the end of the childbearing period of life, age forty-five. Fiftyeight percent of the women who had abortions in 1995 had used a contraceptive method during the month they became pregnant.
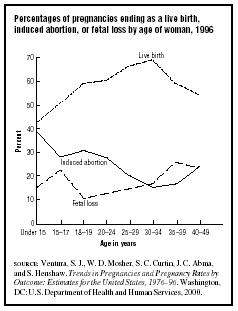
Induced abortion rates vary considerably by age. Figure 1 shows the proportion of pregnancies ending in live births, induced abortion, and fetal loss compared to the age of the woman. Induced abortion rates also differ considerably by race and Hispanic origin. About 16 percent of pregnancies among non-Hispanic white women end in abortion (1 in 6); 22 percent of pregnancies among Hispanic women (1 in 5); and 38 percent of pregnancies among non-Hispanic black women (2 in 5).
On average, women in the United States give at least three reasons for choosing an abortion: three-fourths say that having a baby would interfere with work, school, or other responsibilities; approximately two-thirds say that they cannot afford to have a child; and half say that they do not want to be a single parent or are having problems with their husband or partner. Support for abortion varies considerably by social class, with support consistently increasing by income and education.
For more than two centuries in early U.S. history (from the 1600s to the early 1900s), abortion was not a crime if it was performed before quickening (fetal movement, which begins at approximately twenty weeks). An antiabortion movement began in the early 1800s, led by physicians who argued against the validity of the concept of quickening and who opposed the performing of abortions by untrained people, which threatened physician control of medical services. The abortion controversy attracted minimal attention until the mid-1800s when newspapers began advertising abortion preparations. Opponents of these medicines argued that women used them as birth control measures and that women could also hide extramarital affairs through their use. The medicines were seen by some as evidence that immorality and corruption threatened America. By the early 1900s, virtually all states (at the urging of male politicians; women could not vote at the time) had passed antiabortion laws.
In the landmark 1973 case Roe v. Wade, the U.S. Supreme Court made abortion legal by denying the states the right to regulate early abortions. The court conceptualized pregnancy in three parts (trimesters) and gave pregnant women more options in regard to abortion in the first trimester (three months) than in the second or third trimester. The court ruled that during the first trimester the abortion decision must be left to the judgment of the woman and her physician. During the second trimester, the right to abortion remained but a state could regulate certain factors in an effort to protect the health of the woman, such as the type of facility in which an abortion could be performed. During the third trimester, the period of pregnancy in which the fetus is viable outside the uterus, a state could regulate and even ban all abortions except in situations in which they were necessary to preserve the mother's life or health.
The controversy over abortion in the United States did not end with the Supreme Court's decision, but rather has intensified. Repeated campaigns have been waged to overturn the decision and to ban abortion altogether. Although the high court has continued to uphold the Roe decision, support for abortion rights has decreased with the appointment of several conservative judges.
A New York Times /CBS News Poll taken twenty-five years after Roe v. Wade found that the majority of the American public still supports legalized abortion but says it should be harder to get and less readily chosen. Some observers call this a "permit-but-discourage" attitude. Overall, 32 percent of the random sample of 1,101 Americans in the poll said abortion should be generally available and legal; 45 percent said it should be available but more difficult to obtain; and 22 percent said it should not be permitted.
Physical and Emotional Aspects of Abortion
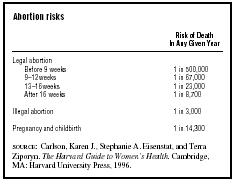
The chance of dying as a result of a legal abortion in the United States is far lower than the chance of dying during childbirth. Before the nine-week point in pregnancy, a woman has a one in 500,000
| Abortion risks | |
|
Risk of Death
In Any Given Year |
|
| Legal abortion | |
| Before 9 weeks | 1 in 500,000 |
| 9–12 weeks | 1 in 67,000 |
| 13–16 weeks | 1 in 23,000 |
| After 16 weeks | 1 in 8,700 |
| Illegal abortion | 1 in 3,000 |
| Pregnancy and childbirth | 1 in 14,300 |
|
SOURCE
: Carlson, Karen J., Stephanie A. Eisenstat, and Terra
Ziporyn. The Harvard Guide to Women's Health. Cambridge, MA: Harvard University Press, 1996. |
|
chance of dying as a result of an abortion. This compares to a one in 14,300 chance of dying as a result of pregnancy and childbirth (see Table 1). Infection is a possibility after an abortion, but longterm complications such as subsequent infertility, spontaneous second abortions, premature delivery, and low birthweight babies are not likely.
Some women experience feelings of guilt after an abortion, while others feel great relief that they are no longer pregnant. Still other women are ambivalent: They are happy to not be pregnant, but sad about the abortion. Some of these emotional highs and lows may be related to hormonal adjustments and may cease after the woman's hormone levels return to normal. The intensity of feelings associated with an abortion usually diminish as time passes, though some women may experience anger, frustration, and guilt for many years.
Those experiencing severe, negative psychological reactions to abortion are rare, according to research findings reviewed by a panel commissioned by the American Psychological Association. The panel wrote, "the question is not simply whether abortion has some harmful psychological effects, but whether those effects are demonstrably worse than the psychological consequences of unwanted childbirth." Women experiencing distress could find comfort in talking with loved ones, sensitive and trusted friends, and professional counselors experienced in working with abortion issues.
See also: Bioethics ; Black Stork ; Children, Murder OF ; Infanticide ; Mortality, Childbirth ; Mortality, Infant
Bibliography
Adler, Nancy E., et al. "Psychological Factors in Abortion: A Review." American Psychologist 47 (October 1992):1194–1204.
Alan Guttmacher Institute. Sharing Responsibility: Women, Society and Abortion Worldwide. New York: Author, 1999a.
Alan Guttmacher Institute. Induced Abortion Worldwide. New York: Author, 1999b.
Alan Guttmacher Institute. Into a New World: Young Women's Sexual and Reproductive Lives. New York: Author, 1998.
Alan Guttmacher Institute. Hopes and Realities: Closing the Gap between Women's Aspirations and Their Reproductive Experiences. New York: Author, 1995.
Boston Women's Health Book Collective. Our Bodies, Ourselves for the New Century: A Book By and For Women. New York: Touchstone/Simon & Schuster, 1998.
Brody, J. E. "Abortion Method Using Two Drugs Gains in a Study." New York Times, 31 August 1995, A1.
Francoeur, Robert T., ed. International Encyclopedia of Sexuality. New York: Continuum, 1997.
Goldberg, C., and J. Elder. "Poll Finds Support for Legal, Rare Abortions." Lincoln Journal Star, 16 January 1998, 1.
Hausknecht, Richard U. "Methotrexate and Misoprostol to Terminate Early Pregnancy." New England Journal of Medicine 333, no. 9 (1995):537.
Hyde, Janet Shibley, and John D. DeLamater. Understanding Human Sexuality, 7th edition. Boston: McGraw-Hill, 2000.
Insel, Paul M., and Walton T. Roth. Core Concepts in Health, 8th edition. Mountain View, CA: Mayfield, 2000.
Kelly, Gary F. Sexuality Today: The Human Perspective, 7th edition. Boston: McGraw-Hill, 2001.
Landers, S. "Koop Will Not Release Abortion Effects Report." American Psychological Association Monitor (March 1989):1.
Olson, David H., and John DeFrain. Marriage and the Family: Diversity and Strengths, 3rd edition. Mountain View, CA: Mayfield, 2000.
Strong, Bryan, Christine DeVault, and Barbara Werner Sayad. Human Sexuality: Diversity in Contemporary America, 3rd edition. Mountain View, CA: Mayfield, 1999.
Winikoff, Beverly, and Suzanne Wymelenberg. The Whole Truth about Contraception. Washington, DC: National Academy of Sciences, 1997.
Internet Resources
Alan Guttmacher Institute. "Abortion in Context: United States and Worldwide." In the Alan Guttmacher Institute [web site]. Available from www.agi-usa-org/pubs/ib_0599.htm
Alan Guttmacher Institute. "Induced Abortion." In the Alan Guttmacher Institute [web site]. Available from www.agi-usa-org/pubs/fb_induced_abortion.html
National Opinion Research Center (NORC). "General Social Surveys." In the NORC [web site]. Available from www.norc.org/projects/gensoc.asp
JOHN DeFRAIN
A CCIDENTS
See C AUSES OF D EATH ; I NJURY M ORTALITY .
Comment about this article, ask questions, or add new information about this topic: